In many health systems, anesthesia staffing stability is measured by whether the day runs as planned. When volume rises, add-ons accumulate, or clinicians need more flexibility, leaders are balancing access, performance, and workforce expectations in real time. Coverage may be achieved, but often through continuous adjustment.
At ASA ADVANCE, Medicus hosted a panel on how health systems can move from managing anesthesia staffing strain to building greater stability. Leaders from Endeavor Health shared practical perspectives on strategies they've implemented to support coverage and reduce reliance on short-term fixes.
Panelists Included
 |
Mohammed Minhaj, MD, MBA, FASA, FACHEHarris Family Foundation Chair, Department of Anesthesiology, Critical Care and Pain Medicine, NorthShore, Swedish, and Northwest Community Hospitals |
 |
Matthew BelangerSystem Vice President, Surgical Services & Anesthesia at Endeavor Health |
 |
Francesco Sessa, MS, MBA, CRNAChief Nurse Anesthetist at Endeavor Health |
Understanding How Organizations Are Currently Supporting Coverage
To ground the conversation in the current reality, session attendees were asked how their organizations typically support anesthesia coverage during staffing challenges.
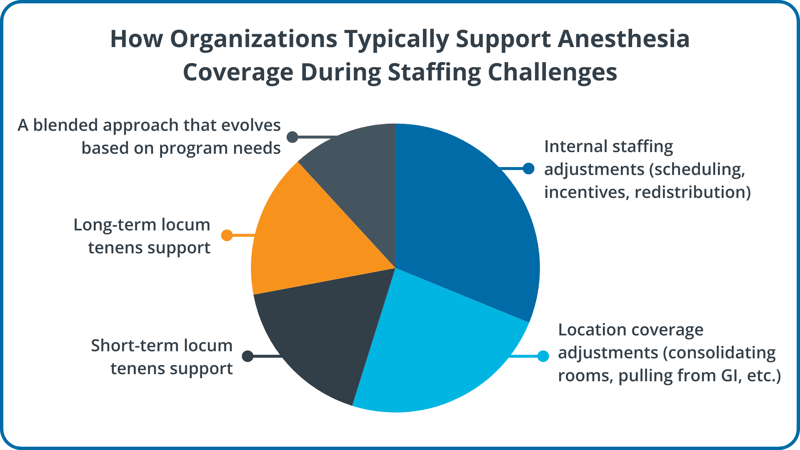
Taken together, the responses reflected a common dynamic in today’s environment: leaders are pulling multiple levers at once to protect OR access, often with limited margin for disruption.
Protecting Access with an Anesthesia Care Team Model
As anesthesia shortages and rising demand continue to challenge leaders, anesthesia care team models were described as a practical lever for maintaining access and reducing day-to-day fragility. The panelists emphasized their value in moments that demand real-time response, including emergencies, late schedule changes, and unexpected shifts in acuity.
Sessa described the anesthesia care team model as creating options in the moment, particularly when the day changes and support is needed quickly.
“It really allows us to have incredible flexibility when that emergency comes in, and we have the ability to move things around staffing in the moment,” Sessa said.
From an operating perspective, the model was discussed less as a staffing workaround and more as a way to build flexibility into daily coverage so teams can adjust without relying on improvised solutions.
Dr. Minhaj pointed to measurable operational outcomes following the implementation of an anesthesia care team at a hospital site, describing performance gains that built confidence and momentum over time.
“The hospital had its highest number of cases ever,” Dr. Minhaj said, adding that “it wasn’t just a one-time success because we built upon that.”
How the Medicus Transition Program Supported the Shift to an Anesthesia Care Team Model
Sessa also described what it looked like to implement staffing changes during a large expansion. With 30 anesthesia locations to cover, the internal work required to coordinate staffing, vet providers, and push credentialing became difficult to sustain alongside broader leadership responsibilities.
“We thought we’d just scale what we had learned in the past,” Sessa said, but “very quickly we learned that was impossible.”
He described how moving to an exclusive, project-based approach through the Medicus Transition Program helped reduce administrative strain and allowed leadership to focus on broader priorities, including culture, alignment, and long-term direction rather than being consumed by day-to-day staffing logistics.
“The Medicus Transition Program… was a game changer because then we could focus on the vision of the culture for this new department and not just sort of the administrative passes,” Sessa said.
Using Technology and Data to Shift Staffing Decisions From Reactive to Planned
Care team models create flexibility, but sustaining stability also depends on planning discipline. Throughout the session, technology and data were described as tools that help leaders anticipate repeatable variability, align stakeholders around shared constraints, and make staffing and capacity decisions with greater intention.
Dr. Minhaj emphasized how data can clarify which operational assumptions hold up and which do not. In his example, utilization data helped reset expectations and focus improvement efforts before expanding capacity further.
“The data shows that on average they’re running a half a case per day, so we’re trying to get to 1 case per day per room before we really tackle the issue of two cases in a room,” he said.
He also described using historical patterns to identify predictable periods of overstaffing and redesign coverage prospectively. The goal was not simply to reduce staffing but to protect coverage while improving predictability for clinicians and leaders.
Belanger approached the topic from the perspective of system operations, emphasizing that metrics matter most when leaders choose the right ones and apply them consistently. He highlighted room utilization as a more reliable signal than block utilization alone, particularly when released time is not consistently backfilled.
“Room utilization is probably my North Star when I’m thinking about this category,” Belanger said.
He also described the operational work that sits behind that metric, including release and backfill practices and reviewing performance across different time windows. In combination, these practices were discussed as a way to reduce avoidable surprises and make coverage planning more predictable.
Looking Ahead
The ASA ADVANCE discussion reflected a reality many anesthesia leaders are navigating: staffing stability is increasingly tied to operating model decisions, not just staffing levels. In Endeavor Health’s experience, care team models supported daily flexibility and access when conditions changed quickly, while data-supported planning helped leaders align around shared constraints and improve predictability over time.
Additional takeaways from the ASA ADVANCE discussion will be explored in future posts, including flexibility as a retention lever, feedback loops that sustain change, and onboarding strategies that support long-term stability.
Interested in learning more about the Medicus Transition Program? Complete the short form below to connect with a Medicus recruiter.